Walk-In With Pain. walk-Out Without Pain
Interventional Pain Management is a comprehensive diagnostic, therapeutic and management service for chronic, acute, and cancer pain. Treatment is provided on an outpatient basis with a structured, time limited program specific to the patient’s individual needs. Interventional pain management involves specialized procedures to treat and manage pain. These might include an injection of a local anesthetic or steroid around nerves, joints, or muscles; spinal cord stimulation; insertion of a drug delivery system; or radiofrequency ablation to stop pain for an extended period of time.
- Back Pain
- Neck Pain
- Joint pain (knee Pain)
- Cancer Pain
- Trigeminal neuralgia
- Sciatica
- Osteoid Osteoma
State-of-the-art fluoroscopically equipped interventional pain management suite is used to provide access for patients in an efficient manner. Available procedures include:
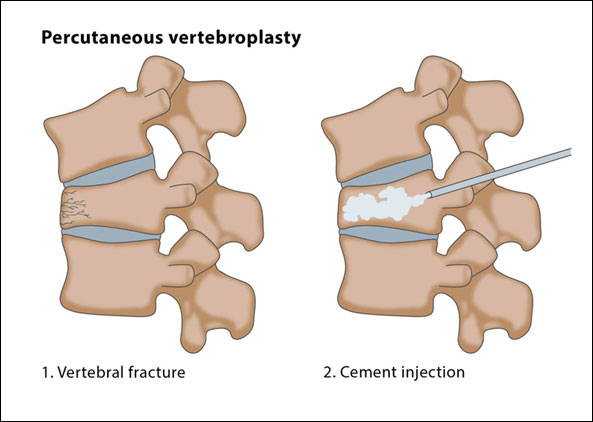
- Percutaneous Vertebroplasty and Kyphoplasty:
Vertebroplasty and kyphoplasty are interventional radiology procedures in which bone cement is injected through a small hole in the skin (percutaneously) into a fractured vertebra with the goal of relieving back pain caused by vertebral compression fractures.
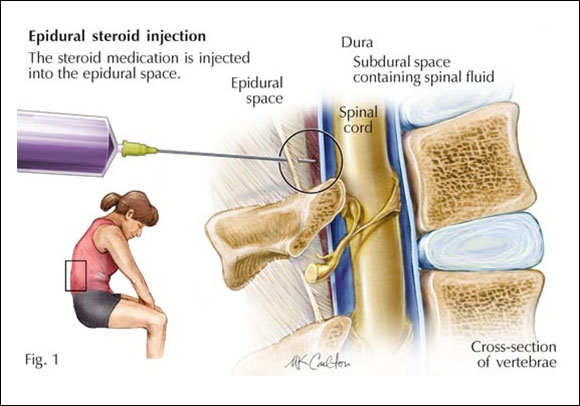
- Epidural injections (in allareas of the spine):
The use of anesthetic and steroid medications injected into the epidural space to relieve pain or diagnose a specific condition.
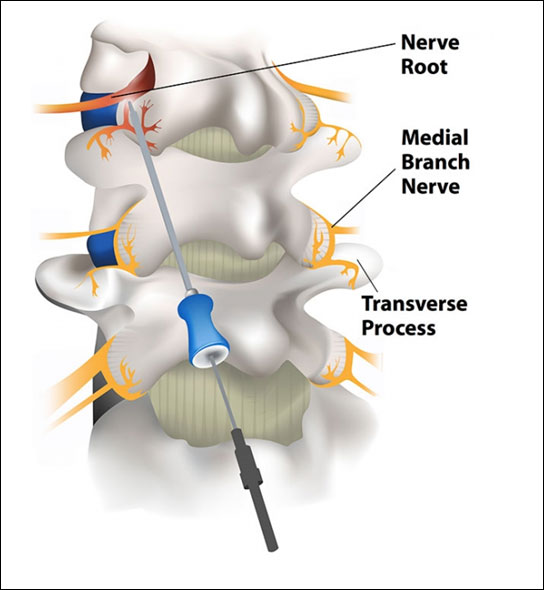
- Selective Nerve, root, and medial branch blocks:
Injections done to determine if a specific spinal nerve root is the source of pain. Blocks also can be used to reduce inflammation and pain.
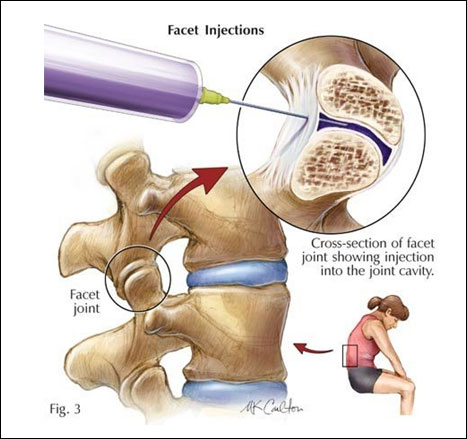
- Facet joint injections:
An injection used to determine if the facet joints are the source of pain. These injections can also provide pain relief.
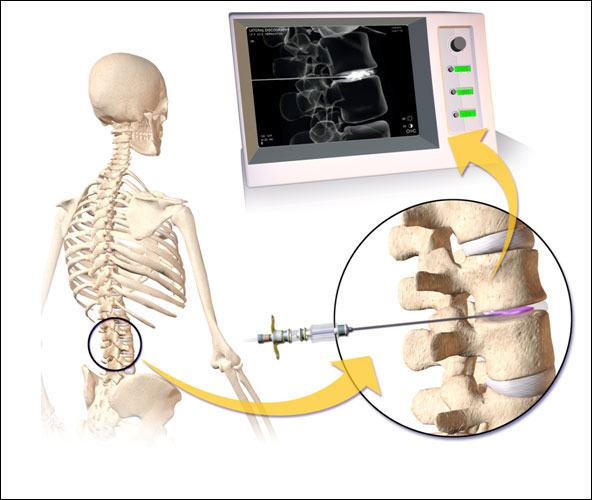
- Discography and Disc Injection:
An “inside” look into the discs to determine if they are the source of a patient’s pain. This procedure involves the use of a dye that is injected into a disc and then examined using x-ray or CT scan.
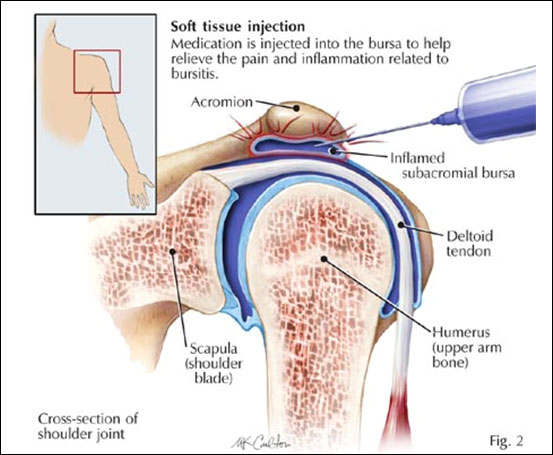
- Articular interventions in pain management:
Chronic joint pain due to rheumatoid arthritis and osteoarthritis.
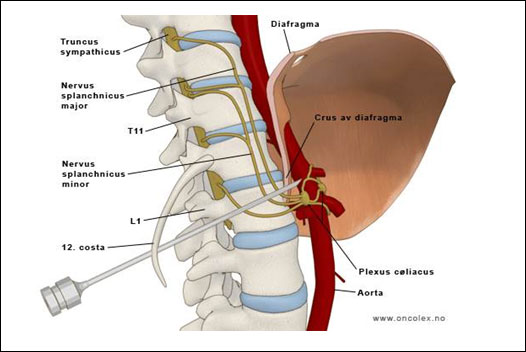
Percutaneous Management of Visceral pain:
Celiac Plexus Block is a useful interventional pain management procedure done in upper abdominal malignancy like; pancreatic cancer, hepato-biliary cancer, primary or secondary cancer of liver etc. and chronic pancreatitis & other chronic pancreatico-biliary diseases. It may be permanent (neurolytic) with alcohol or phenol or temporary with local anaesthetics and depo-steroids. It is performed percutaneously, either under fluoroscopic or CT guidance.Ganglion Impar Block can be performed to treat pain from a rectal or perineal location
Cancer pain:
Percutaneous ablation or Embolisation of painful Neoplasms to relive pain.
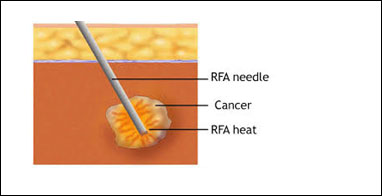
Radiofrequency ablation of Osteoid Osteoma:
Osteoid osteoma is a benign tumor of the bone affecting children and young adults.Treated with Minimally Invasive Technique of Radiofrequency Ablation

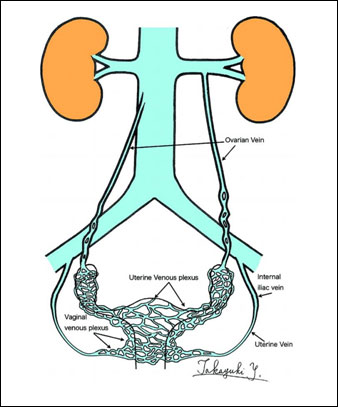
Chronic pelvic pain in women:
Ovarian vein embolization is a minimally invasive treatment for pelvic congestion syndrome, a painful condition resulting from the presence of enlarged or varicose veins in the pelvis.
- Sympathetic nerve block:
A sympathetic nerve block can be used to diagnose or treat pain involving the nerves of the sympathetic nervous system. Examples of conditions for which a sympathetic nerve block might be used include: Pain from spasms in the blood vessels, Complex regional pain syndrome, Raynaud’s syndrome.

It has a number of benefits for patients
- Rapid relief from symptoms.
- The imaging techniques allow accurate diagnosis and treatment using cutting-edge equipment. Diagnosis is reconfirmed during procedure.
- Minimally invasive procedures are performed through a small hole in the skin, minimising the patient’s discomfort and recovery time. There won’t be any scar.
- Most procedures can be performed on an outpatient basis or require only a short hospital stay. As interventional procedures tend to require only local anaesthesia, hospital stays are very short, with patients frequently going home the day the procedure is performed.
- Patients who undergo IR procedures experience less pain during and after the procedure than patients undergoing surgical procedures. Post-procedural care is provided, along with follow-up imaging to confirm if the treatment has been successful.
- Minimal damage to surrounding vital anatomical structures with no significant structural weakness.
- No or negligible blood loss. No requirement of blood transfusion.
- Return to work and other normal activities usually within the first few days after the procedure.
- Low risk compared to surgery. The techniques can be used in very sick patients who are unfit for surgery.
- Overall procedure is less expensive than surgery or other alternatives.
